By Rachel Manuel Bruns

While we see regular news coverage about challenges accessing maternal health care in Iowa and the related racial disparities, I rarely see the mention of higher cesarean rates as a relevant factor in these disparities.
April is Cesarean Awareness Month and April 11-17 is Black Maternal Health Week. The overlap of these initiatives is relevant given the higher cesarean rate for Black people across the country and Iowa.
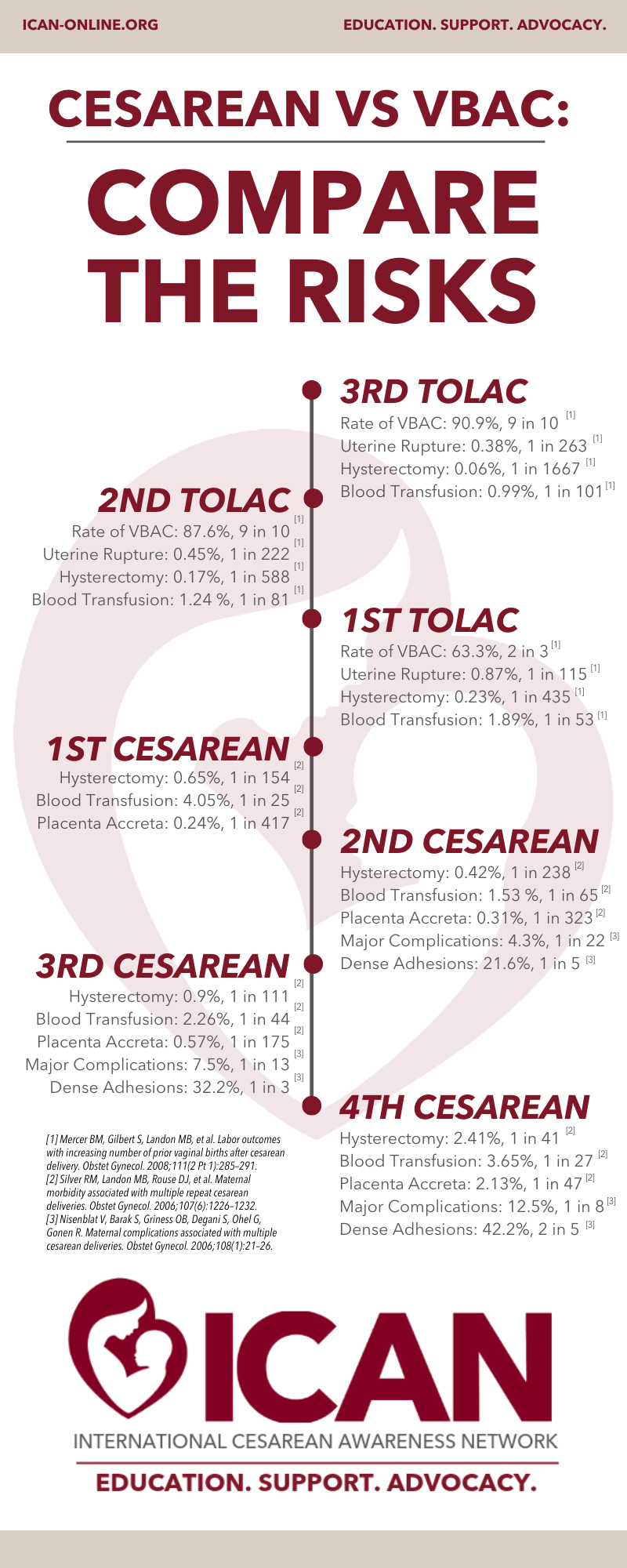
A C-section is worth the risks involved when the health of the birthing parent or baby is at risk. Complications including hemorrhage, infection and organ injury are more likely to occur with a cesarean compared with a vaginal delivery and studies show C-sections are 80% more likely to have complications than vaginal deliveries. Each cesarean also increases the risk for placenta accreta, a serious and life-threatening condition.
CDC data shows the U.S. cesarean delivery rate in 2021 increased to 32.1%, while Black women continued to have the highest cesarean delivery rate at 36.8%. Iowa’s 2020 total cesarean rate was 30.2%, while Black women had a rate of 33.9%, with an overall state low-risk cesarean rate of 24.7% and 30.1% for Black women.
The WHO has reported that cesarean rates higher than 10% are not associated with reductions in maternal and newborn mortality rates. To summarize a 2019 U.S. News & World Report column, in the past 50 years the U.S. has decided to intervene with major abdominal surgery 500% more often, term infants have become 0% better off, and pregnant people have become 50% more likely to die.
Recently released CDC data shows maternal mortality in the United States rose by 40% in 2021. You read that correctly – 40%. That is outrageous. Of course, COVID is a factor in this increase; however, COVID exacerbated an existing maternal health crisis.
The U.S. maternal mortality rate is 10 times higher than other high-income countries like Australia. Countries with lower maternal mortality tend to have more midwives, lower C-section rates and universal health care.
I started my journey learning and advocating for maternal health after my own low-risk cesarean and subsequent vaginal birth after cesarean (VBAC), where I had to drive two hours for supportive care. Iowa’s VBAC rate is 16.8%, but there is room for improvement.
The Iowa Maternal Quality Care Collaborative recently completed a voluntary training safety bundle on reducing first-time cesareans, of which 43 of the state’s 56 hospital birthing facilities participated. Initial data reported shows a 16% reduction in the statewide low-risk cesarean rate. Which hospitals participated in the bundle and annual hospital cesarean rates are not available publicly at this time.
The American College of Obstetrics and Gynecology, the national association setting practice guidelines for OB-GYNs, reaffirmed in its 2017 VBAC practice guidelines that it is reasonable for most people with a previous cesarean scar. Some hospitals in Iowa ban VBACs, essentially telling patients they will only provide prenatal care for repeat cesareans and don’t offer informed consent detailing both the risks and the benefits of a trial after cesarean and planned repeat cesareans.
The ACOG also says that having a suspected big baby, going beyond 40 weeks, having a short birth interval, having a low vertical or unknown scar, expecting twins or having a high BMI are not reasons to rule out planned VBACs. It also cites induction, augmentation, epidural and external cephalic version as options during planned VBACs. These are all worth mentioning, because many of these are restrictions that physicians in Iowa will impose on patients seeking VBAC care.
The ACOG’s current practice guidelines recommend that trial of labor after cesareans be attempted in facilities that can provide cesarean delivery (which would include Level 1 hospitals) for situations that are immediate threats to the life of the woman or fetus. If a hospital with labor and delivery is not safe and able to provide emergency cesareans for VBAC, then how can it provide cesareans for any other birth?
Sharing all this data about VBAC and hospital maternal levels of care may not seem relevant, yet Iowa hospitals continue to take actions that will increase cesarean rates and in turn affect maternal mortality and morbidity.
I continue to be disappointed in Iowa’s medical community that spends time lobbying against bills that would improve access to maternal health care and/or allow problematic practices to continue in hospitals while simultaneously participating in forums discussing the maternal health disparities.
Many providers in Iowa continue to use the VBAC calculator, which was intended as an educational tool and is instead being used as a screening tool to determine if a patient can access the practice. Another medical screening tool frequently used to “risk out” obstetrics patients and possibly unnecessarily increase medical interventions like cesareans is the body mass index, which has a racist history and is not evidence-based.
The recent news from MercyOne Des Moines announcing the elimination of their midwives program will have an impact on VBAC access and cesarean rates in Des Moines. MercyOne was one of the few options for VBAC care, and research shows the midwifery model of care results in fewer C-sections, saves lives and reduces racial disparities.
The economic reality for hospitals is that certified nurse midwives are reimbursed at only 85% of the physician rate for the same work by Iowa Medicaid, which covers 40% of births. While the global reimbursement for Medicaid needs to increase to better reimburse hospitals and all provider types, the state is currently disincentivizing hospitals from staffing midwives by not providing pay parity for the same work.
Some hospitals across Iowa have limited the access to midwives by not allowing midwives to care for VBAC patients or breech patients, which is in their scope of practice. Iowa is ranked 42nd for midwifery integration, which is associated with improved birth outcomes. This limitation on midwives in hospital settings emphasizes the importance of improving access to midwives in out-of-hospital settings, both birth centers and home birth.
I have written extensively about the need to remove birth centers from the certificate-of-need law and the importance of licensing certified professional midwives. This legislative session, a bill passed the Iowa Senate that would reform certificates of need, exempting birth centers. There is also an active lawsuit against the state for imposing the certificate-of-need law on birth centers. Iowa is one of only a few states that currently have zero stand-alone birth centers.
HF 265, which would license certified professional midwives, passed the full House chamber and the Senate State Government and Ways and Means committees. We now wait to see whether it will hopefully advance to the Senate floor for debate and passage.
The Maternal Health Hub recently released an issue brief that said patients should have the ability to access all provider types, including OB-GYNs, family physicians, certified nurse midwives, certified professional midwives, certified midwives and others. It also said the high intervention medical model is not superior to the traditional model that views pregnancy and childbirth as a natural process that does not require intensive intervention.
Those opposed to the midwifery licensure bill, including the Iowa Hospital Association, the Iowa Medical Society and physician groups, want an amendment that would limit the scope of certified professional midwives to not allow them to attend VBAC, breech or twin births, which are within the training and scope of certified professional midwives. With over a dozen certified professional midwives currently attending these births in Iowa, limiting their scope would end up harming pregnant people and likely result in increased maternal mortality and morbidity.
The irony of this is that if OB-GYNs and hospitals did not want home births to happen for VBACs or breech births, then they could start providing that care themselves, as currently it is difficult to find supportive vaginal birth after cesarean care, and there are no hospitals providing vaginal breech care in the state. Approximately 1 in 25 patients will be breech. In what other medical profession is it acceptable to not be trained for 1 in 25 patients?
While I am an advocate for increasing access to midwives, I fully recognize the importance of having access to physicians and fortunately Iowa has some phenomenal physicians trained in obstetrics. That being said, when comparing the U.S. to other high-income countries with significantly better maternal health outcomes, midwives, which do not have to be nurses, significantly outnumber OB-GYNs.
If you are an obstetrics provider, the scope of practice of another profession is not a threat to you, especially in the current environment where Iowa is ranked 11th as a maternal health desert and is currently experiencing an OB-GYN shortage, which is predicted to only get worse.
I support the initiatives by Gov. Kim Reynolds to fund rural OB fellowships and provide funding for regional models of care. However, the effective implementation of this funding is critical to ensure success and actually improve maternal health outcomes. The funding should go to hospitals that are following practice guidelines for vaginal birth after cesareans and to hospitals that have demonstrated they have cesarean rates that are not excessively high. Unfortunately, as currently implemented this has not been the case.
Reading about maternal health can often be depressing given the continued and alarming rise in mortality and morbidity. If you are pregnant, avoid consuming these negative stories when possible. Seek out stories of positive birth experiences and take charge of your own birth education. If you’re feeling overwhelmed, reach out to a peer support group like ICAN, Postpartum Support International or the Black Doula Collective Parent Support Group.
If you are involved in birth work, I urge you to check out the Evidence Based Birth resources on Anti-Racism in Health Care and Birth Work.
Rachel Manuel Bruns is a maternal health advocate and chapter leader for the International Cesarean Awareness Network (ICAN) of Central Iowa. Professionally, Rachel is chief engagement officer for America’s Service Commissions, which supports national service and volunteering throughout the country. She lives in Des Moines with her partner and two children. Rachel can be contacted at rachel.m.bruns@gmail.com.



{kind=link}